


The Mirage of Long COVID: When Methodology Trumps Sensationalism

In an age awash with misinformation, our friends Trafcy Høeg, Vinay Prasad, and Shamez Landi serve as the intellectual lifeboat for those drowning in the murky waters of long COVID research. With the precision of a surgeon's scalpel, they dissect the prevailing epidemiological studies, revealing a disconcerting anatomy of error and bias. The authors expose how the current case definitions, as broad as they are bewildering, have been erroneously employed by esteemed health organizations. These definitions have metamorphosed into a Pandora's box, liberating a host of symptoms as attributable to long COVID without even a modicum of evidential support
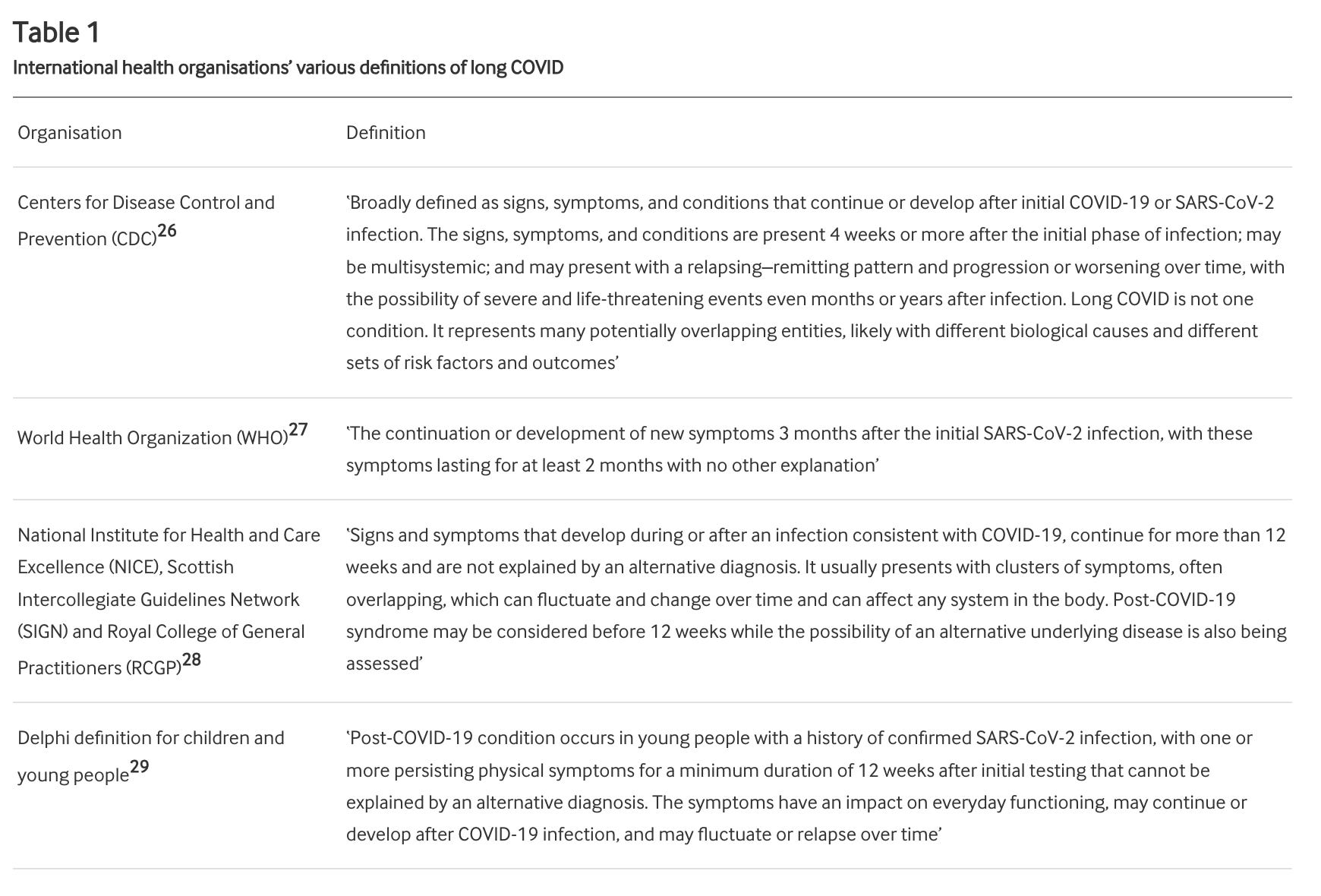
The authors don't merely cast aspersions; they offer a solution. They advocate for a more nuanced case definition that demands temporally aligned symptoms post a laboratory-confirmed COVID-19 diagnosis, effectively weeding out alternative culprits. They argue that this strategy will prevent the medical community from chasing ghosts—phantom symptoms erroneously attributed to long COVID.
Yet, the greatest sin committed by current research, the authors contend, is the startling omission of appropriate control groups. With only 11% of studies incorporating such controls, the risk assessments of persistent symptoms lack a critical yardstick. In the absence of this comparative baseline, these estimates flutter about in a scientific abyss, bereft of substantive meaning.
The authors go on to reveal the impact of rigorous methodology. When studies are tightly controlled, the inflated numbers of long COVID cases deflate like a pricked balloon. For instance, a high-caliber UK study showed a minuscule 1.6% difference in symptom prevalence between the infected and matched controls. This robust evidence also nullifies the myth of heightened long COVID risk among adults under 50 and children at 12 weeks post-infection.
The study casts its critical gaze beyond the immediate issues, pointing out pervasive selection and sampling biases. Like a distorted mirror, these biases skew the reflection of reality, further exacerbating the problem of inaccuracy. The authors persuasively argue that this methodological maelstrom has whipped up an unwarranted storm of societal anxiety and clinical hypervigilance.
In their denouement, Høeg et al. underscore the dire need for methodological rectitude. They posit that only through such rigor can we navigate the labyrinthine complexities of long COVID, steering clear of the Scylla and Charybdis of overdiagnosis and mistreatment. Their critique emerges as a lighthouse, guiding the ship of scientific inquiry through treacherous waters towards the safe harbor of empirical truth.
In sum, the article is a magnum opus of scrutiny, unearthing the systemic flaws that have plagued our understanding of long COVID. It is a clarion call for a sea change in research standards, one that could recalibrate the compass guiding clinical practice and public health policy. It is, in my considered opinion, a tour de force that will indelibly influence the discourse on this most pressing intersection of science, medicine, and society.
Long covid is very rare indeed however what a great way of covering up millions of people disabled and injured by the bioweapon aka "the vaccine". Next they will tell us long covid is causing people to vote the wrong way so we should not be allowed to vote!
Seems to me many of the symptoms of long Covid are similar to those of depression and anxiety. Considering how we have been treated since 2020, I would think depression and anxiety would be running rampant in the population. Just my opinion.