


The Ultimate List: mRNA Vaccines + Myocarditis
The evidence is now OVERWHELMING - a very real risk to kids, young adults and possibly all ages.

I stand on the shoulders of giants - or probably just the shoulder of people who have a lot more time on their hands than I do. Regardless, I’m fairly adept at digesting and cataloguing the pantheon of studies about all things Covid. (See our post last week on children)
Let’s take all of this to heart - it’s an unfortunate pun but we need to bring serious attention to the MASSIVE wave of studies showing that the mRNA vaccines can indeed cause a debilitating disease like myocarditis.
Did y'all catch that the FDA finally got around to publishing the data signals on the mRNA vaccine? - Risk of lung clots up 50% - Risk of heart attacks up 40%+ They knew the signals were there and did nada.

Let’s define this disease:
Myocarditis is a condition in which the heart muscle, also called the myocardium, becomes inflamed. This inflammation can cause the heart muscle to become weakened, stiff, or enlarged, which can lead to problems with the heart's ability to pump blood effectively.
My grandpa was an MD and there’s a reason I am not. I get squeamish when I look at innards so I’m just going to link to this video that
posted and add a little blackout square - you choose! But it shows what anyone can tell is a very damaged heart:
But let’s get to the studies and get you the details you need to counter the myocarditis-deniers out there.
First our quick one-liner summaries for your tweeting pleasure:
FDA finally admits in its own report on 65+ mRNS recipients: Risk of lung clots up 50% - Risk of heart attacks up 40%+ https://www.sciencedirect.com/science/article/pii/S0264410X22014931
Jan 2022, JAMA study found myocarditis risk increased in multiple age, sex groups after mRNA COVID-19 vaccination, highest in young men. https://jamanetwork.com/journals/jama/fullarticle/2788346
Study of VAERS data between Jan-Jun 2021 found highest rate of myocarditis in young boys 12-15 after dose 2 of mRNA COVID-19 vaccination. https://onlinelibrary.wiley.com/doi/10.1111/eci.13759
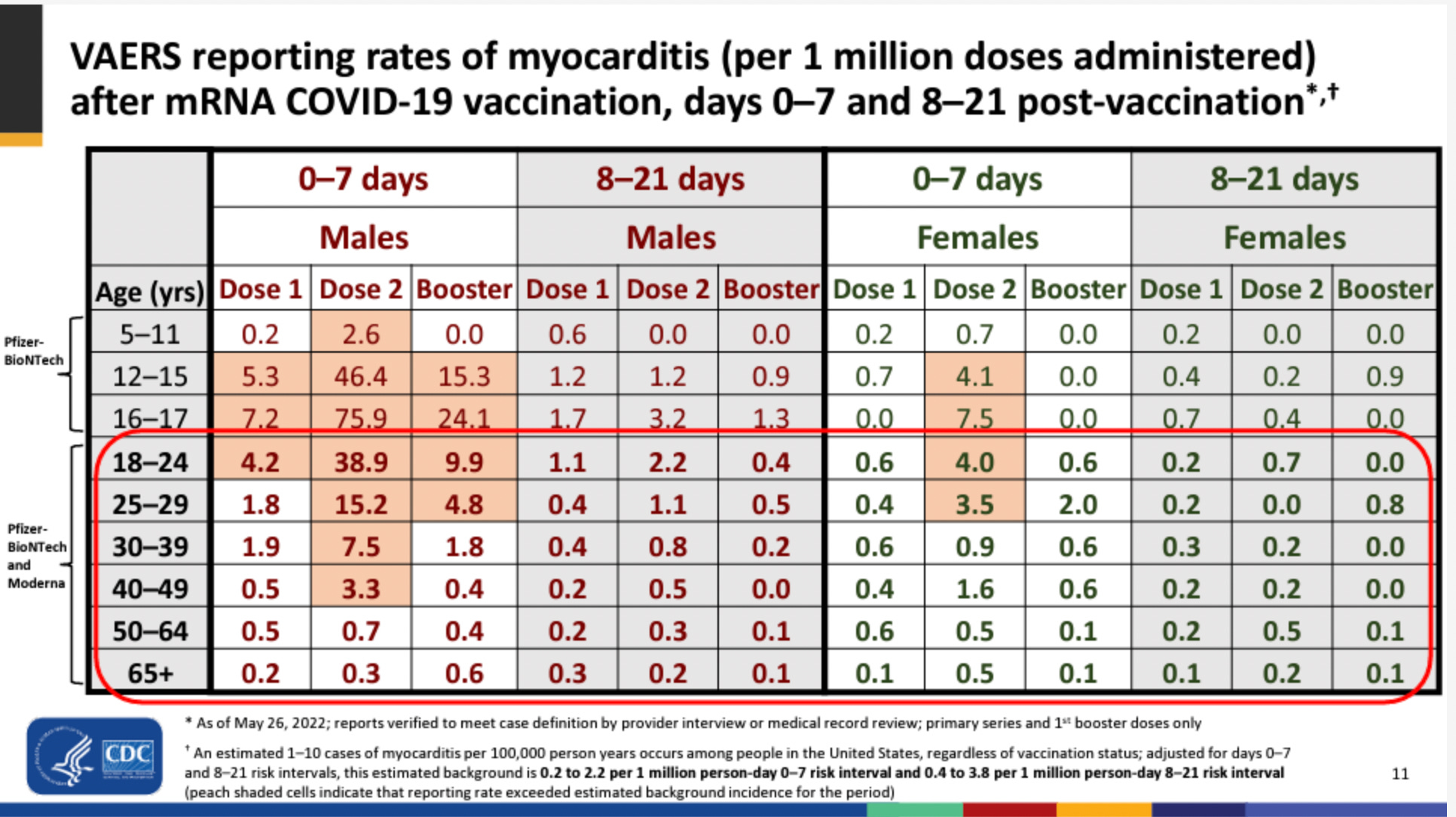
This slide presentation to the CDC and FDA on myocarditis should have rung some IMMEDIATE alarms bells - but we went on vaxxing the young lads anyway. https://fda.gov/media/159007/download
Study in Nature found increased risks of myocarditis and pericarditis in France after Covid-19 mRNA vaccines, particularly after 2nd dose and in age 18-24 yrs, both male and female were affected. https://www.nature.com/articles/s41467-022-31401-5
CDC report 2022 found 14 cases of myocarditis or pericarditis among 102,091 males aged 16-17 who received Pfizer-BioNTech Covid-19 vaccine, significant departure from reported rates in 2021, showing concerns labeled as misinformation are real. https://thefederalist.com/2022/09/09/cdc-admits-post-vaccine-myocarditis-concerns-that-were-labeled-covid-misinformation-are-legit/
Study found myocarditis/pericarditis as rare side effect of mRNA COVID-19 vaccines, disproportionately affects young male adolescents, commonly after 2nd dose of primary series and 1st booster. https://www.acpjournals.org/doi/10.7326/M22-2274
The estimated MMRRs and SMR were about 4 times higher than the MMRRs and SMR. The study concludes that the SARS-CoV-2 vaccine is associated with a higher risk of myocarditis death in all age groups, including the elderly. The risk may be 4 times or higher than the apparent risk of myocarditis death. https://www.medrxiv.org/content/10.1101/2022.10.13.22281036v1.full.pdf
Markedly elevated levels of full-length spike protein were detected in the plasma of individuals with post-vaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects. It suggests that the cause of myocarditis may be linked with spike antigen. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.122.061025
The risk ratio for the mRNA vaccines combined is 1.43 which means that recipients are 43% more likely to have a serious adverse event. https://www.sciencedirect.com/science/article/pii/S0264410X22010283
You’re going to have to vax 35K young adults to prevent one hospitalization and in doing so you’re going to send nearly 20 of these folks into a serious adverse reaction from the vax. https://jme.bmj.com/content/early/2022/12/05/jme-2022-108449
First Studies
First, we must give big kudos to Tracy Beth Høeg, Allison Krug, Josh Stevenson, & John Mandrola.
in particular risked he career to call this out as early of as March of 2021. She would go on to lead one of the first retrospective studies with Rational Ground’s own . Allison Krug and are two of my favorite docs on Team Reality.SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis
The study used Vaccine Adverse Event Reporting System (VAERS) to conduct a retrospective epidemiological assessment of reports filed between January 1, 2021, and June 18, 2021, among adolescents aged 12-17 who received mRNA vaccination against COVID-19. They used the words chest pain, myocarditis, pericarditis and myopericarditis to identify children with evidence of cardiac injury and the word troponin was a required element in the laboratory findings. They found that the post-vaccination cardiac adverse event rate was highest in young boys aged 12-15 following dose two. For boys 12-17 without medical comorbidities, the likelihood of post vaccination dose two cardiac adverse event is 162.2 and 93.0/million respectively. It exceed their expected 120-day COVID-19 hospitalization rate at both moderate and high COVID-19 hospitalization incidence.
Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021
In January 2022, JAMA network published a peer-reviewed article my Matthew Oster & others. This one covered not just young men but other age strata as well:
This study used the Vaccine Adverse Event Reporting System (VAERS) to describe the reports of myocarditis and the reporting rates after mRNA-based COVID-19 vaccination in the US. Between December 2020 and August 2021, 1626 cases of myocarditis were reported in a national passive reporting system among a total of 354,100,845 mRNA-based COVID-19 vaccines administered to more than 192 million people in the US. The risk of myocarditis after receiving mRNA-based COVID-19 vaccines was increased across multiple age and sex strata and was highest after the second vaccination dose in adolescent males and young men. The median age of those with myocarditis was 21 years, and the median time to symptom onset was 2 days. Males accounted for 82% of the cases. 826 cases of myocarditis among those younger than 30 years of age had detailed clinical information available, and 98% of these cases had elevated troponin levels. 72% had abnormal electrocardiogram results and 72% had abnormal cardiac magnetic resonance imaging results. 96% of these cases were hospitalized, 87% of which had resolution of symptoms by discharge. The study concludes that mRNA-based COVID-19 vaccines are associated with an increased risk of myocarditis across multiple age and sex strata, especially in adolescent males and young men.
CDC reports on myocarditis itself and no one seems to notice
This slide presentation to the CDC and FDA on myocarditis should have rung some IMMEDIATE alarms bells - but we went on vaxxing the young lads anyway.
Age and sex-specific risks of myocarditis and pericarditis following Covid-19 messenger RNA vaccines
Nature Magazine published a study in the same month as the CDC slideshow:
This study aimed to provide a comprehensive assessment of the association between myocarditis and pericarditis and the Covid-19 mRNA vaccines (BNT162b2 [Pfizer–BioNTech] and mRNA-1273 [Moderna]) in France. Using nationwide hospital discharge and vaccine data from May 12, 2021 to October 31, 2021, the study found increased risks of myocarditis and pericarditis during the first week following vaccination, and particularly after the second dose. The adjusted odds ratios for myocarditis of 8.1 (95% CI, 6.7 to 9.9) for the BNT162b2 and 30 (95% CI, 21 to 43) for the mRNA-1273 vaccine. The largest associations were observed for myocarditis following mRNA-1273 vaccination in persons aged 18 to 24 years. The study revealed a substantial burden of both myocarditis and pericarditis across other age groups and in both males and females, due to the mRNA-based Covid-19 vaccines.
CDC Admits Post-Vaccine Myocarditis Concerns That Were Labeled Covid Misinformation Are Legit
Sophia Corso has perhaps the most extensive article about this issue published in The Federalist in Sept 2022. The article states that in 2021, when reports first surfaced that some cases of myocarditis (inflammation of the heart muscle) were potentially associated with the Covid-19 vaccine, the corporate media and its fact-checkers were quick to label them as misinformation, saying the benefits of the vaccine far outweigh its small risks. However, a year later, the media can no longer deny that what they called misinformation actually has data to back it up. According to Vaccine Safety Datalink surveillance data from the Centers for Disease Control and Prevention (CDC), there were 14 verified cases of myocarditis or pericarditis among the 102,091 males aged 16-17 who got the Pfizer-BioNTech vaccine, representing a significant departure from last year's reported rates of myocarditis.
Incidence of Myocarditis/Pericarditis Following mRNA COVID-19 Vaccination Among Children and Younger Adults in the United States
This study aims to estimate the incidence of myocarditis/pericarditis among young people (ages 5-39) following mRNA-based COVID-19 vaccines (Pfizer-BioNTech and Moderna) from December 2020 through August 2022. The study used the Vaccine Safety Datalink (VSD), a collaborative of 8 integrated health care delivery systems, to conduct population-based surveillance for cases of myocarditis/pericarditis within 1-98 days of vaccination. They identified 320 potential cases among 5-39 year-olds, with 224 (70%) of them verified through medical record review. They found that 61% of the verified cases occurred within the first 7 days after vaccination, with 18 cases after the first dose and 119 cases after the second dose. The incidence of myocarditis/pericarditis was higher among males than females and higher among adolescent males aged 12-15 and 16-17. Furthermore, they found that the incidence of myocarditis/pericarditis after the first booster was higher than the second dose of primary series. The study concludes that myocarditis/pericarditis is a rare side effect of mRNA-based COVID-19 vaccines, but disproportionately affects young male adolescents and occurs more commonly after the second dose of primary series and first booster.
SARS-CoV-2 vaccine and increased myocarditis mortality risk: 2 A population based comparative study in Japan
The study investigated the association between the SARS-CoV-2 vaccine and myocarditis death in Japan. It is a population-based comparative mortality study. The study population was 99,834,543 individuals aged 12 years and older who had received the SARS-CoV-2 vaccine once or twice by February 14, 2022. The reference population was defined as persons aged 10 years and older from 2017 to 2019. The primary outcome was myocarditis death, which is defined as death caused by myocarditis, with onset 28 days or less after vaccination. The myocarditis mortality rate ratio (MMRR) and the standardized mortality ratio (SMR) were calculated. The results of the study showed that the MMRR was 4.03 in people in their 20s, 6.69 in people in their 30s, and 3.89 in people in their 40s. The SMR of myocarditis was 2.01 for the overall vaccinated population and 1.65 for people 60 years or older. The estimated MMRRs and SMR were about 4 times higher than the MMRRs and SMR. The study concludes that the SARS-CoV-2 vaccine is associated with a higher risk of myocarditis death in all age groups, including the elderly. The risk may be 4 times or higher than the apparent risk of myocarditis death.
Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis
A study has been conducted on blood samples of 16 adolescents and young adults hospitalized for myocarditis after vaccination with SARS-CoV-2 targeted mRNA vaccines and 45 healthy, asymptomatic, age-matched vaccinated control subjects. The study found that the mRNA vaccine-induced immune responses did not differ between individuals who developed myocarditis and individuals who did not, However, it was found that markedly elevated levels of full-length spike protein were detected in the plasma of individuals with post-vaccine myocarditis, whereas no free spike was detected in asymptomatic vaccinated control subjects. It suggests that the cause of myocarditis may be linked with spike antigen.
COVID-19 vaccine boosters for young adults: a risk benefit assessment and ethical analysis of mandate policies at universities
Some of our favorite Team Reality doctors and researches contributed to this important essay on the cost/benefit of the vaccine for young men.
This study is evaluating the appropriateness of COVID-19 booster mandates for students at North American universities. The study combines an empirical risk-benefit assessment and ethical analysis to evaluate the booster mandates for young adults aged 18-29 years. The study finds that to prevent one COVID-19 hospitalization over a 6-month period, 31,207-42,836 young adults would need to receive a third mRNA vaccine. The study concludes that the booster mandates for young adults may result in a net harm, and is not based on updated stratified risk-benefit assessment for this age group. The study also finds that the harms caused by the mandates, including myopericarditis cases and reactogenicity interfering with daily activities, are not proportionate to the public health benefits and may violate the reciprocity principle.
Comparative Safety of the BNT162b2 Messenger RNA COVID-19 Vaccine vs Other Approved Vaccines in Children Younger Than 5 Years
This study retrospectively evaluated the safety of the BNT162b2 SARS-CoV-2 vaccine in children younger than 5 years old by surveying the guardian-reported safety profiles of the vaccine in 7,806 children. The study found that higher dosages of BNT162b2 were significantly associated with injection-site reactions and that, when compared with non-SARS-CoV-2 vaccines, BNT162b2 was associated with more frequent injection-site, musculoskeletal, dermatologic, or otolaryngologic symptoms but fewer general symptoms and fever after vaccination. Overall, the study found that the overall frequency of adverse events after vaccination with BNT162b2 was comparable to the frequency of adverse events after vaccination with approved non-SARS-CoV-2 vaccines in children younger than 5 years.
Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults
This is a secondary analysis of serious adverse events reported in the Phase III randomized clinical trials of Pfizer and Moderna mRNA COVID-19 vaccines in adults. According to this analysis, the Pfizer and Moderna mRNA COVID-19 vaccines were associated with an excess risk of serious adverse events in comparison to placebo, with an increase of 10.1 and 15.1 per 10,000 respectively. The risk ratio for the mRNA vaccines combined is 1.43 which means that recipients are 43% more likely to have a serious adverse event. The study concludes that the excess risk of serious adverse events found in the study points to the need for formal harm-benefit analyses, particularly those that are stratified according to risk of serious COVID-19 outcomes.
Kaufman Institute for Coincidence
https://youtu.be/hZZFnNwdgqQ
excellent summary. thank you!